
HERITAGE TO HEALTH
Heritage to Health operates a drama group in South London, bringing together student nurses and children with learning disabilities to develop effective communication skills. The initiative aims to enhance communication between these two groups — with the ultimate goal of reducing preventable deaths in hospital settings.
Improving Communication in the Care Sector
Role: Senior UX Researcher & Designer
Deliverable: Research Report & Wirefreames
Impact: Secured programme expansion to the University of East Anglia
Research Challenge: All three stakeholder groups, organisers, nurses, and learning disabled children lacked the information they needed to engage confidently with the programme.
Organisational Context: Ad-hoc manual processes made the programme unsustainable and impossible to scale across UK universities.
01 — The Problem
Poor communication between nurses and learning disabled children has real, documented consequences in hospital settings. Heritage to Health is trying to change that — through a drama group in South London bringing the two groups together to learn how to connect.
The programme was integrated into the nursing syllabus at Kingston University, but the manual organisation process was causing problems. Attendees were dissatisfied and frustrated. Organisers, full-time lecturers fitting this around their day jobs, were overwhelmed. The process was ad-hoc, lacked repeatable structure and was held together by goodwill rather than systems.
The organisation also had ambitions to scale, clearly needing to establish repeatable processes that could be embedded into the nursing syllabus across the UK. The current setup made that impossible.
02 — Research Questions
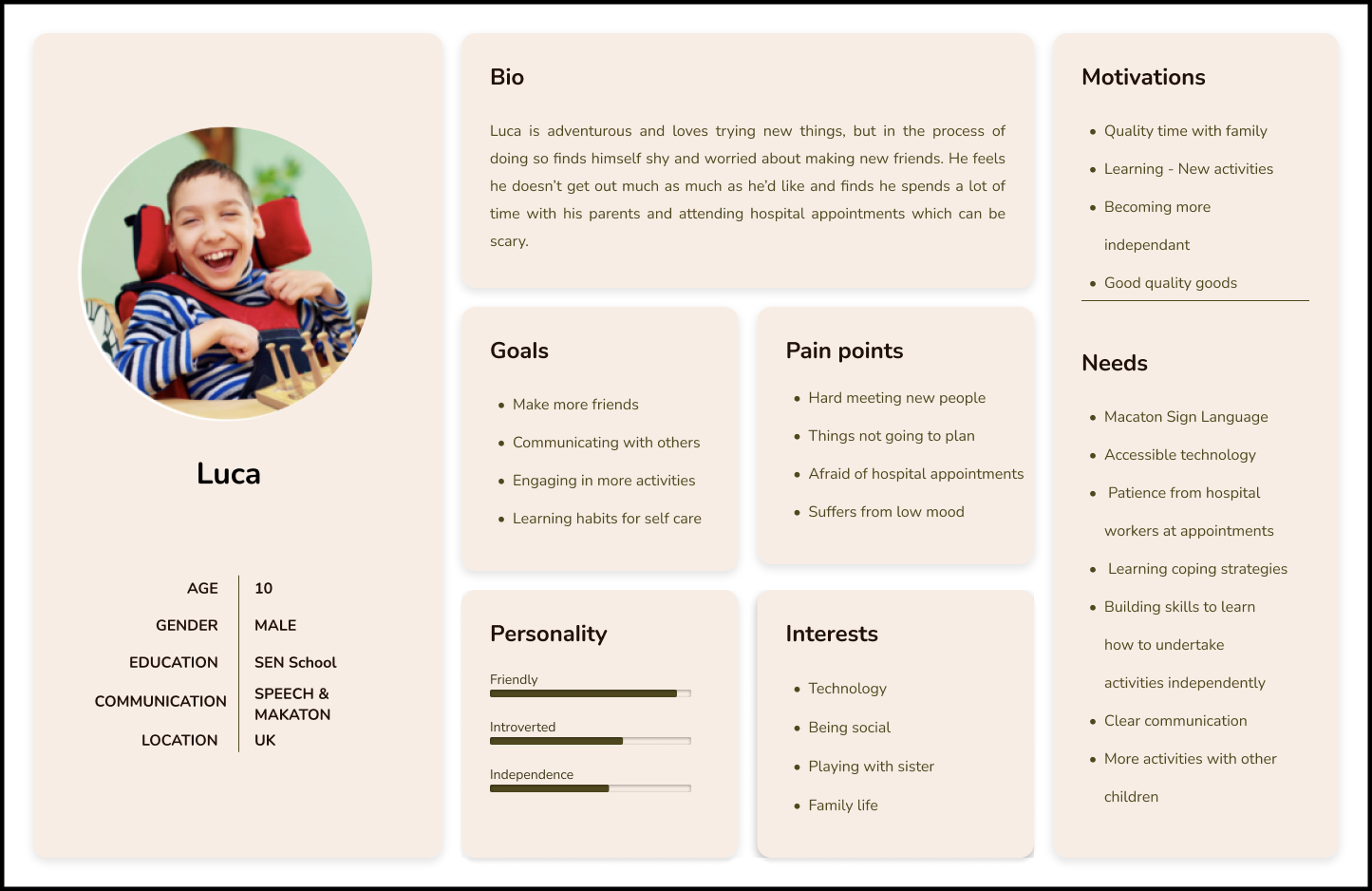
Q1 What are the experiences of learning disabled children within the drama group?
Q2 What are the barriers preventing nurses from engaging confidently with the programme?
Q3 What is the operational burden on organisers and what does it take to scale?
Q4 What does a minimum viable solution look like that serves all three groups?
03 — Methods
Many of the learning disabled children were non-verbal, making user interviews alone an unsuitable method. A mixed-methods approach was essential — combining immersive fieldwork, focus groups, and interviews to build a complete picture across all three stakeholder groups. More detailed information on each study available on request.
8 Week Field Study
The drama sessions moved to Zoom during Covid — a host reading a story while nurses and children engaged with props like masks and flags to build connection. Observing remotely over 8 weeks let me understand the service I was designing for: how it ran, where it worked, and where it didn’t.
For non-verbal children, observation was the only viable research method. Informal Zoom debriefs with parents after each session bridged what I’d observed with lived experience I couldn’t access directly.
Focus Group with Nurses
A focus group with six student nurses was chosen over individual interviews deliberately. Peer validation was key, nurses were more willing to open up when they realised others felt the same way.
Questions were designed to surface the full range of challenges nurses faced, with some framed around what felt personally difficult — creating space for honesty on what could have been a sensitive topic.
Interviews with Organisers
Three one-to-one interviews were conducted with organisers — each holding a slightly different role within the programme. Individual sessions allowed each organiser’s specific responsibilities and pressures to be explored in depth.
Design Sprint (Co-Design)
A design sprint was introduced mid-project in response to scope creep. With the client pushing for features ahead of the research, a structured session was needed to ground decisions in evidence and manage expectations around the MVP.
Two back-to-back sessions brought together the key stakeholders: the lead organiser, the drama lead, a developer to assess viability, a parent as an advocate for the children’s perspective, and myself facilitating. Methods included How Might We questions, dot voting and rapid prototyping — moving from problem framing to prioritised solutions with full transparency on what could realistically be built.

8 week online field study
04 — FINDINGS
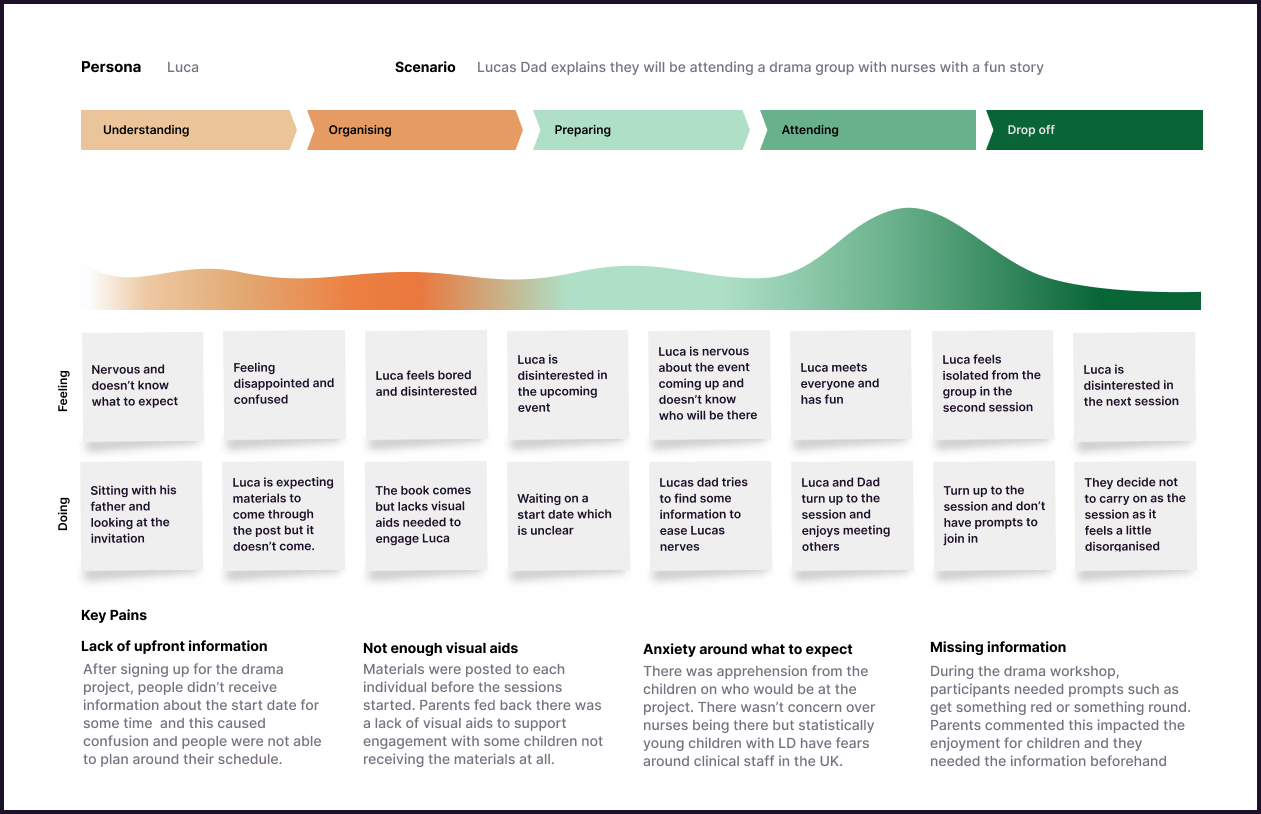
A single thread ran through all three stakeholder groups: no one had the information they needed, when they needed it. This resulted in decreased engagement and anxiety on all sides going into sessions.
The core need was shared, though it looked different for each group. Organisers had no reliable way to communicate logistics. Nurses weren't receiving what they needed to prepare. Children had no visibility on what to expect or who was coming.
Communication was broken across all three groups
Nurses felt fearful of saying or doing the wrong thing. Key information was arriving too late to act on, leaving them without the preparation or context to engage confidently.
Nurses were arriving anxious and underprepared
Many children weren’t receiving their weekly story packs in the post ahead of sessions — materials designed to help them prepare. Some received them, others didn’t, creating inconsistency and disappointment. Knowing what was coming made a measurable difference to how children engaged.
Children needed to know what to expect
The programme was only running because of personal investment that wasn’t sustainable. Without systemised processes, scaling to other universities wasn’t viable.
Organisers were at capacity
Any solution had to be immediately intuitive. Given the diversity of users, complexity in any feature was a direct barrier to inclusion.
Simplicity was non-negotiable
05 — Design
The feature set was determined through co-design with all stakeholders and scoped tightly around the core MVP. Four features were taken forward — each chosen to reduce a specific burden on organisers while directly serving the needs of nurses and children.
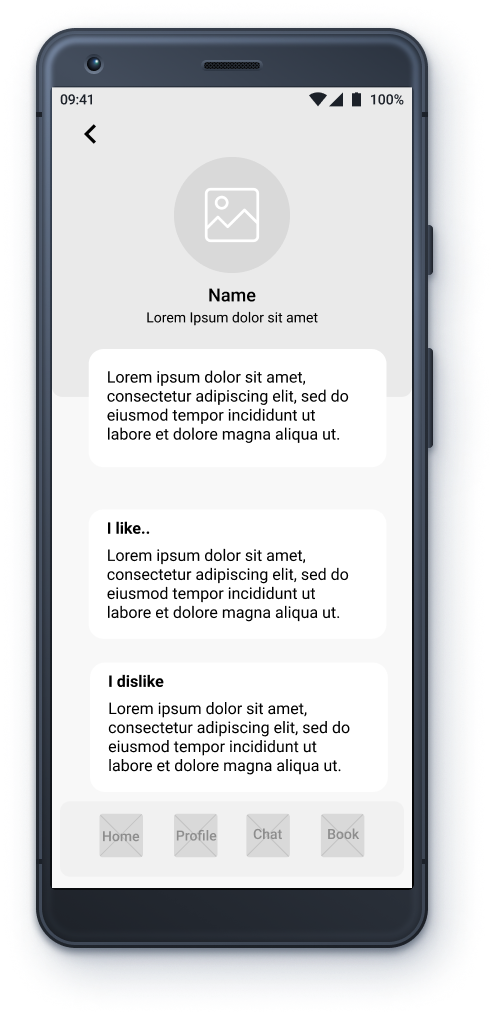
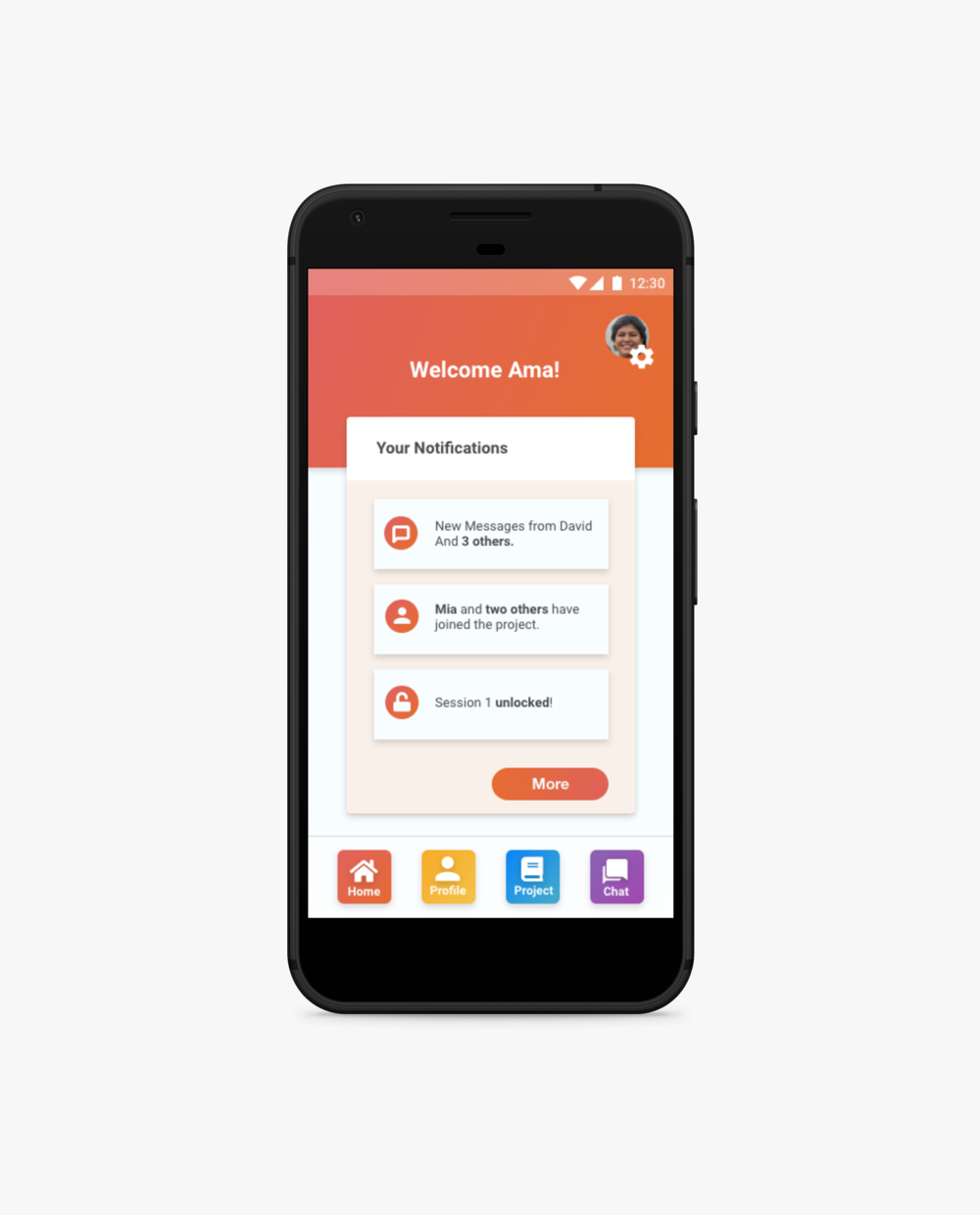
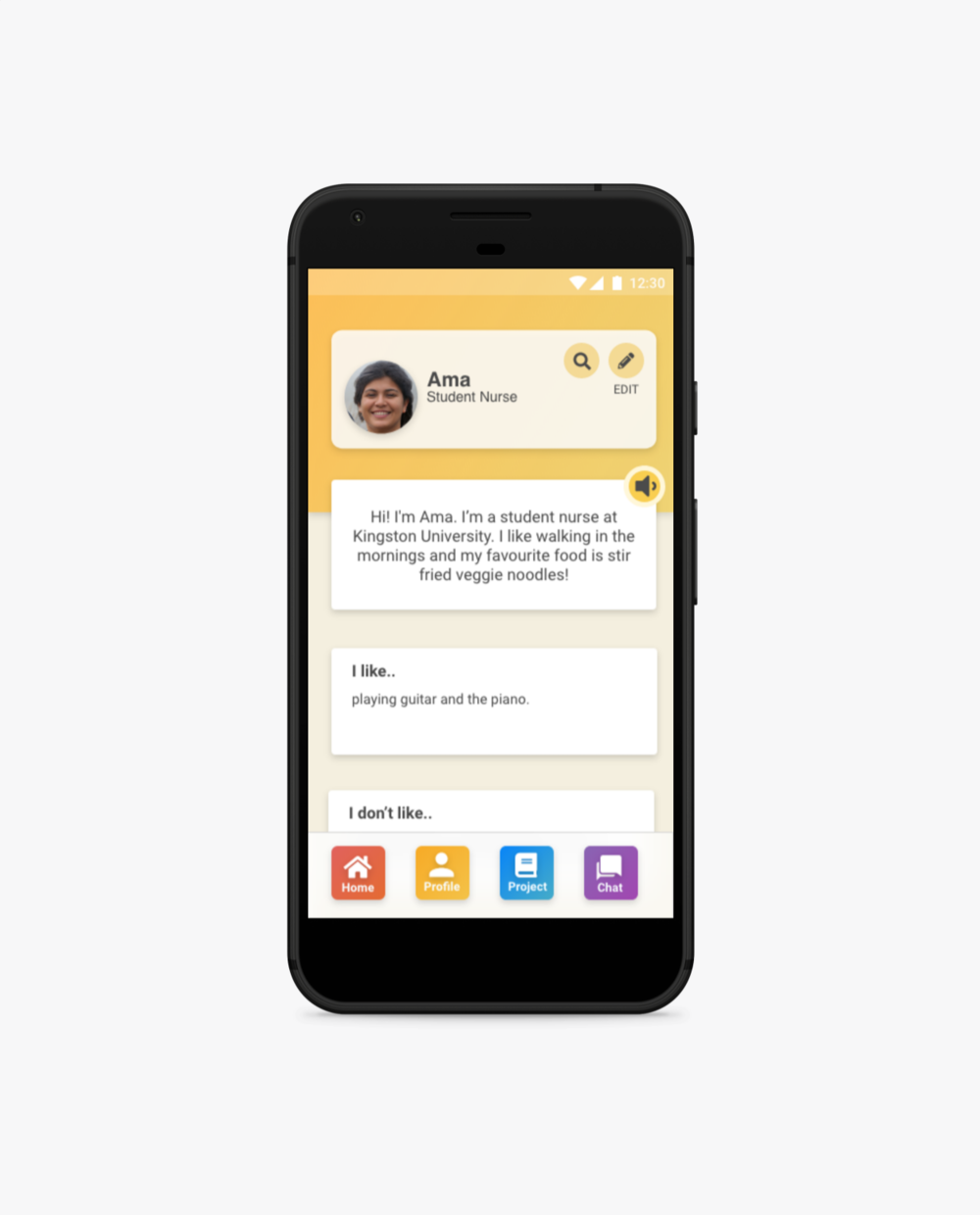
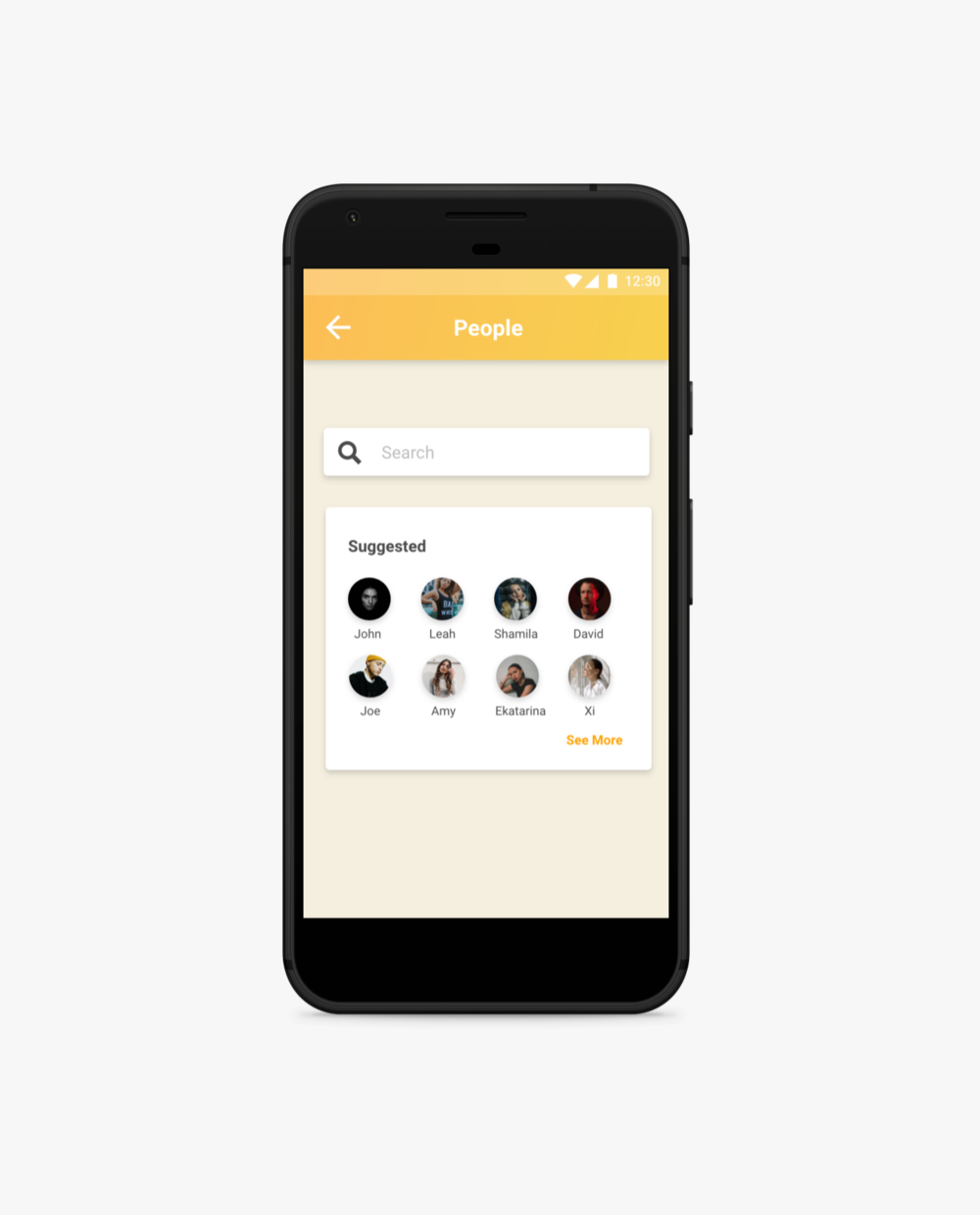
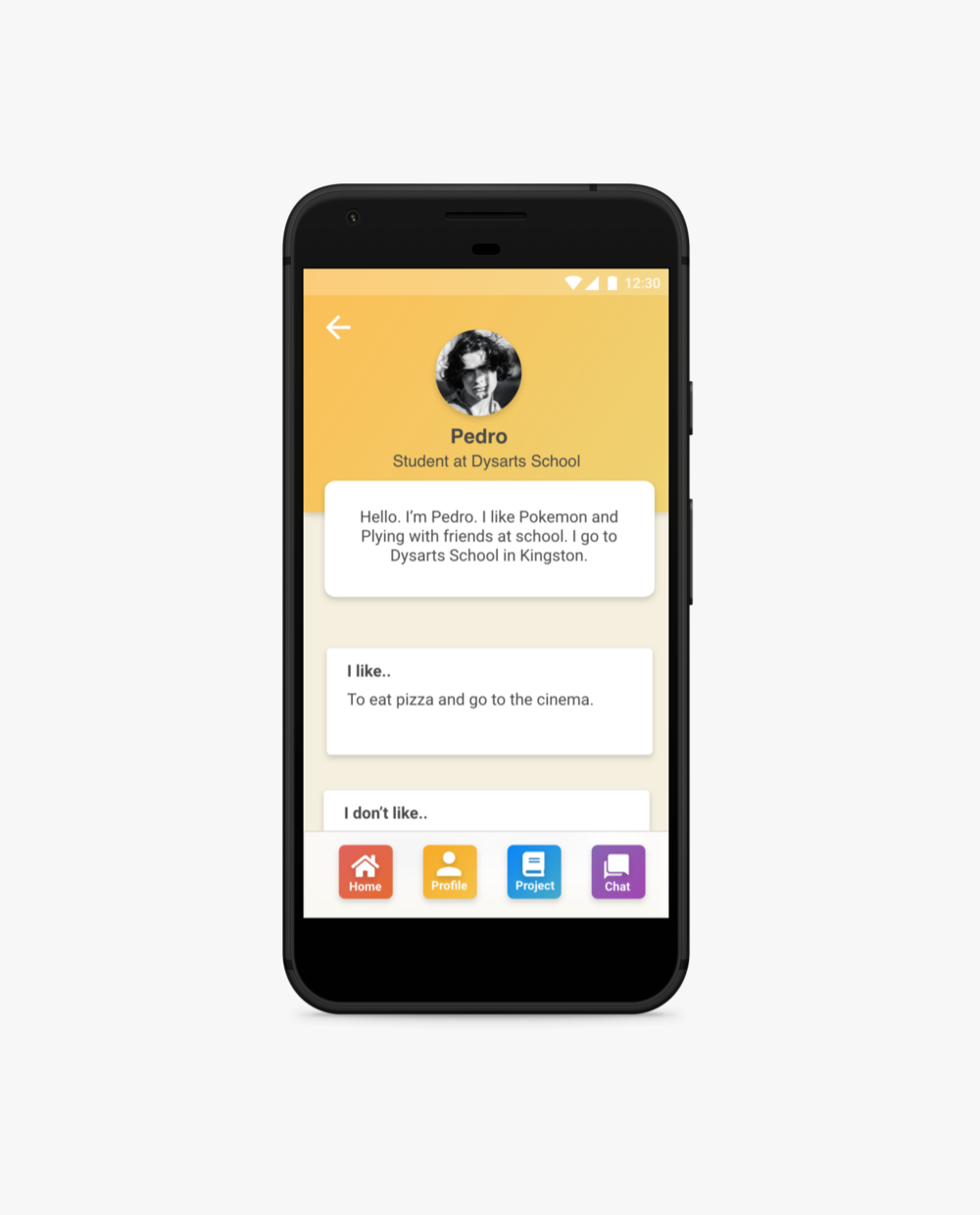
Profile Section
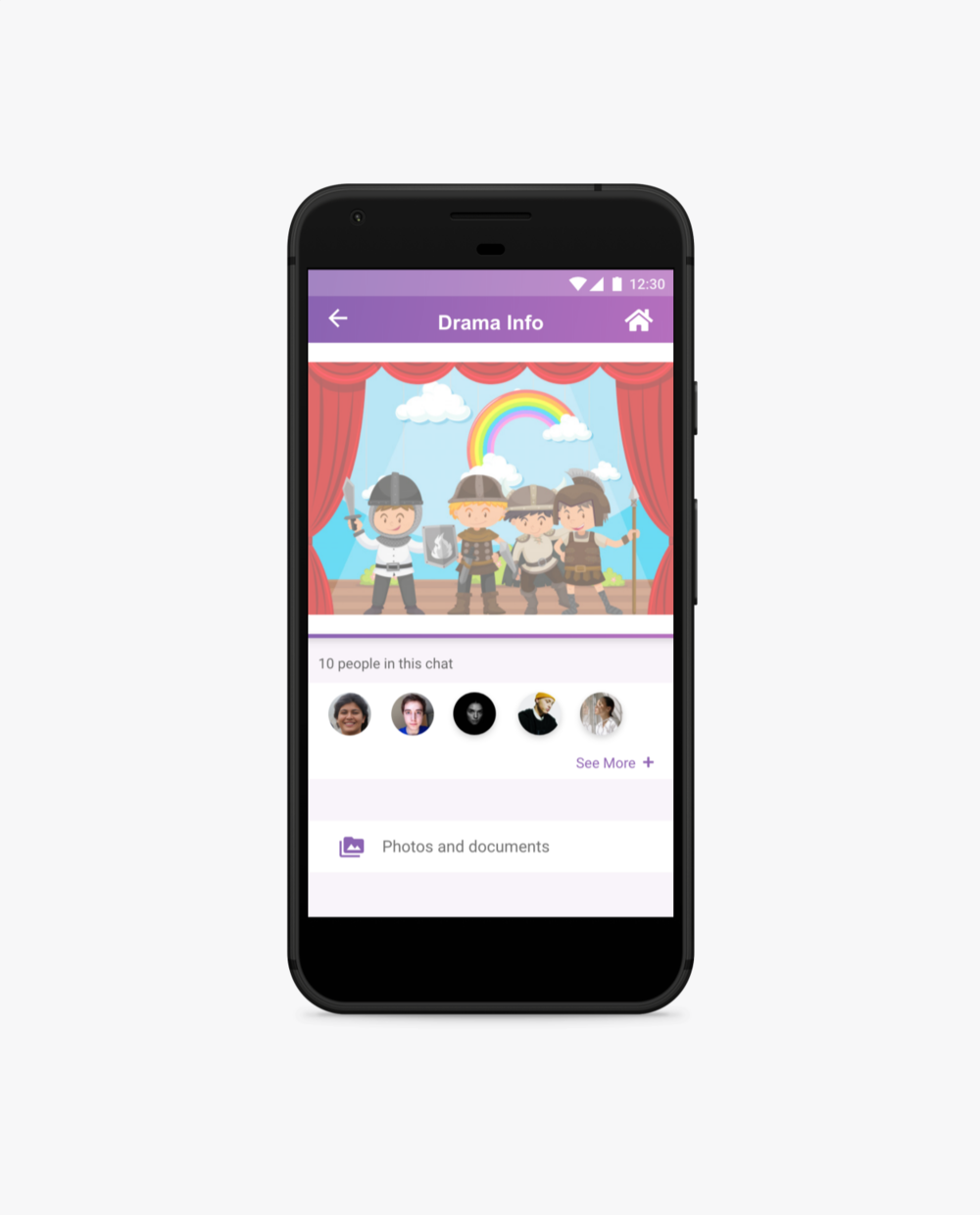
Allowed nurses to understand the children's individual needs before attending the group, reducing anxiety and improving preparedness. Equally gave children visibility on who would be attending — supporting positive anticipation rather than fear of the unknown.
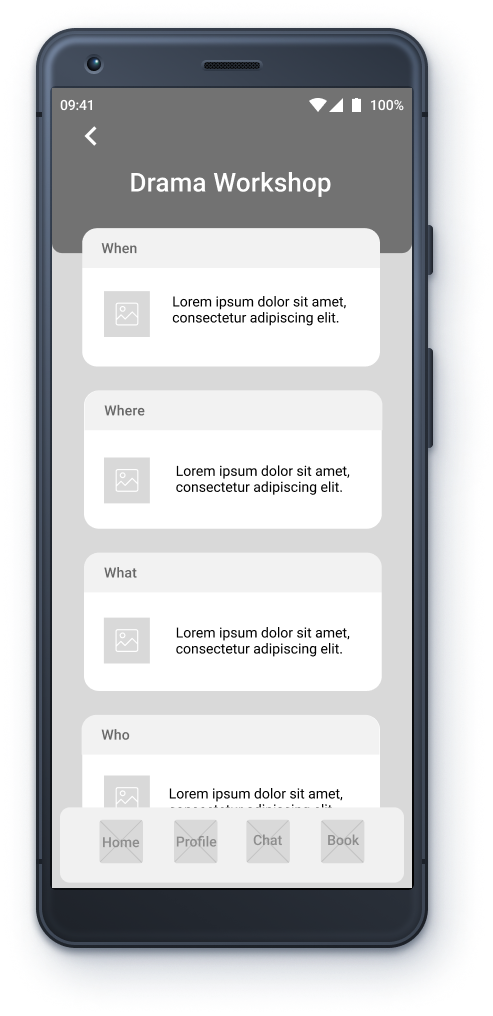
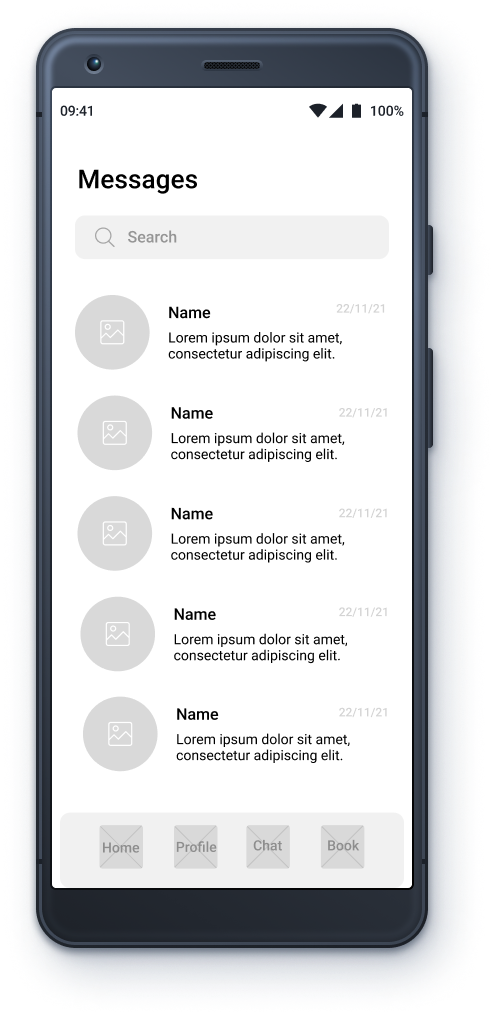
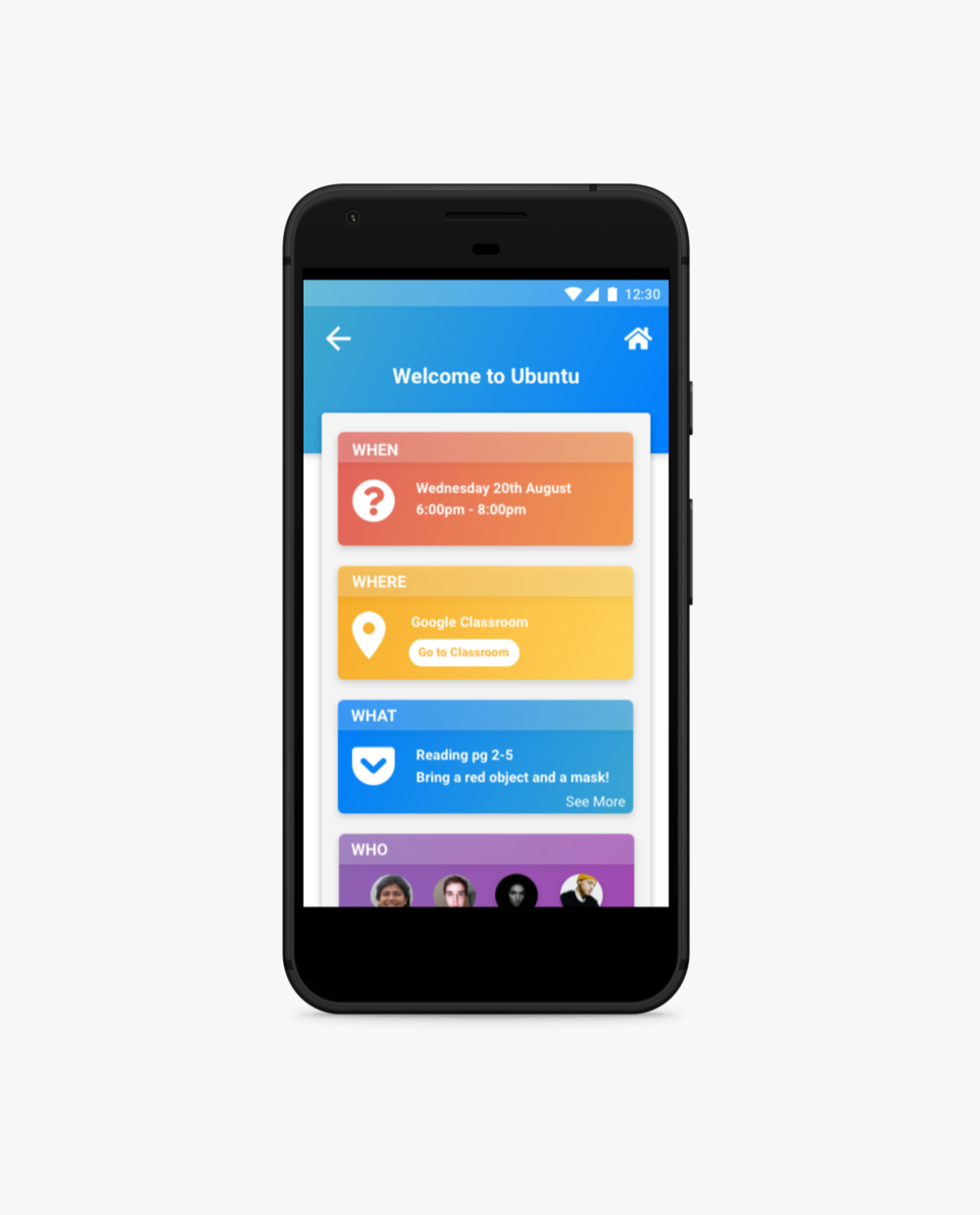
Events Page
A calendar was considered but ruled out — with sessions running quarterly, it would have been overkill for an MVP. A simple events page gave organisers and participants what they actually needed: clear, timely information without unnecessary complexity.
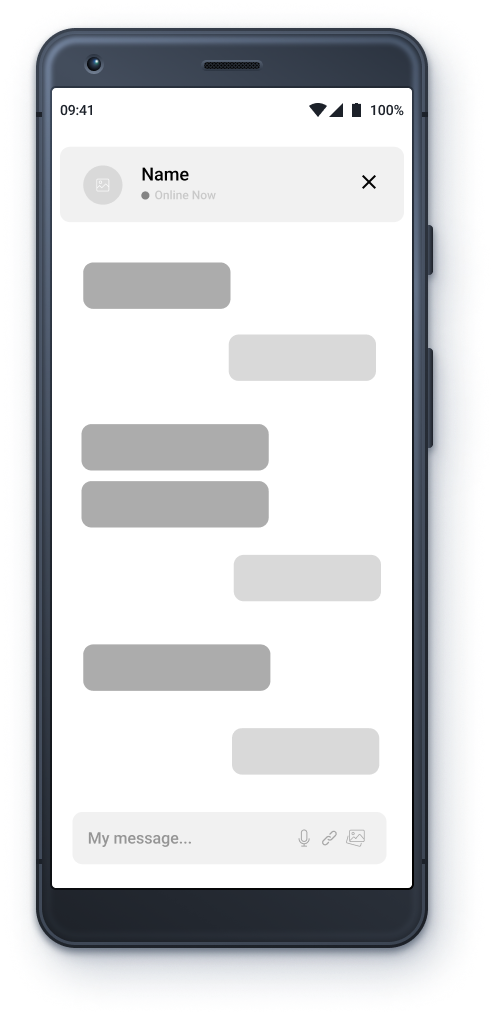
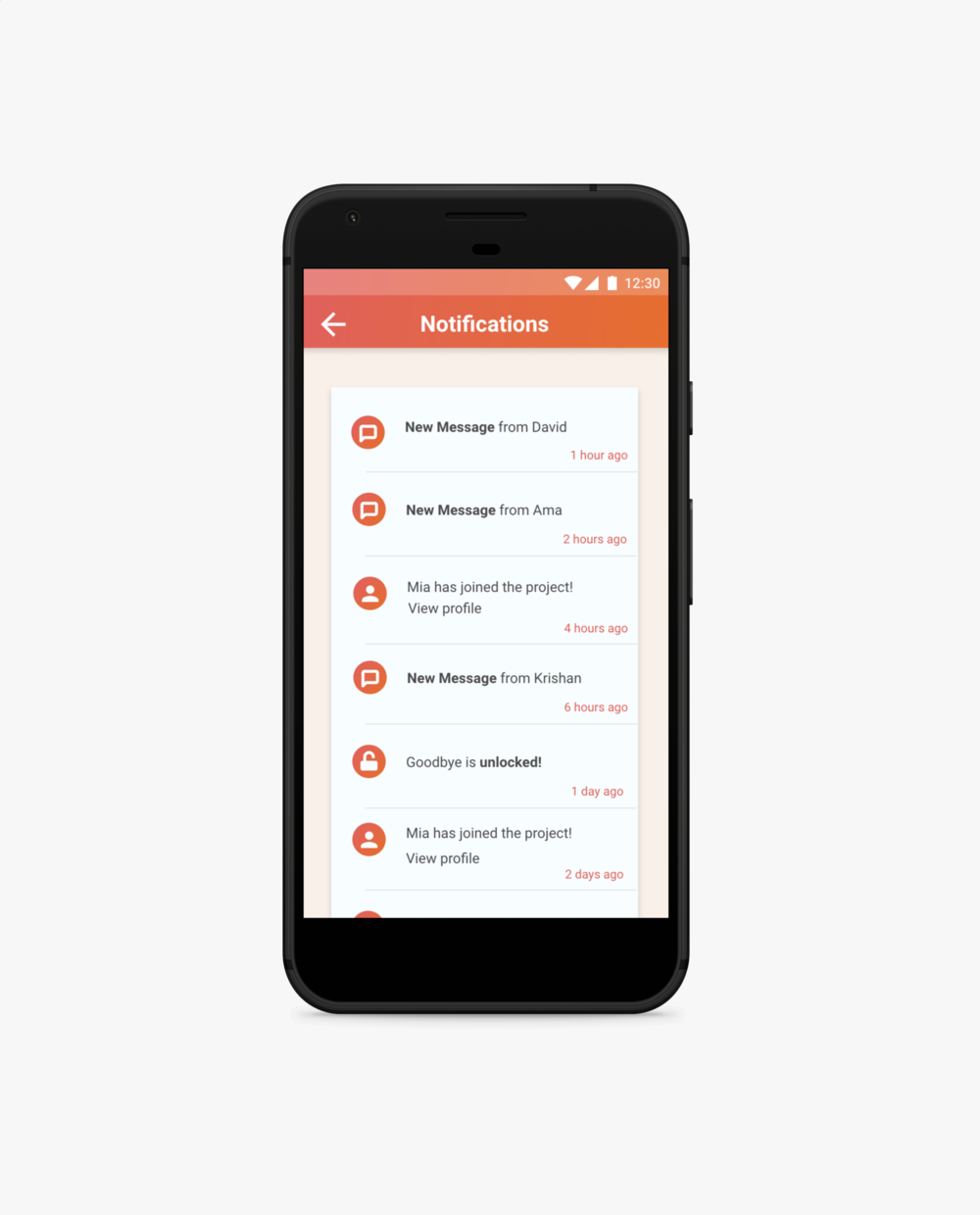
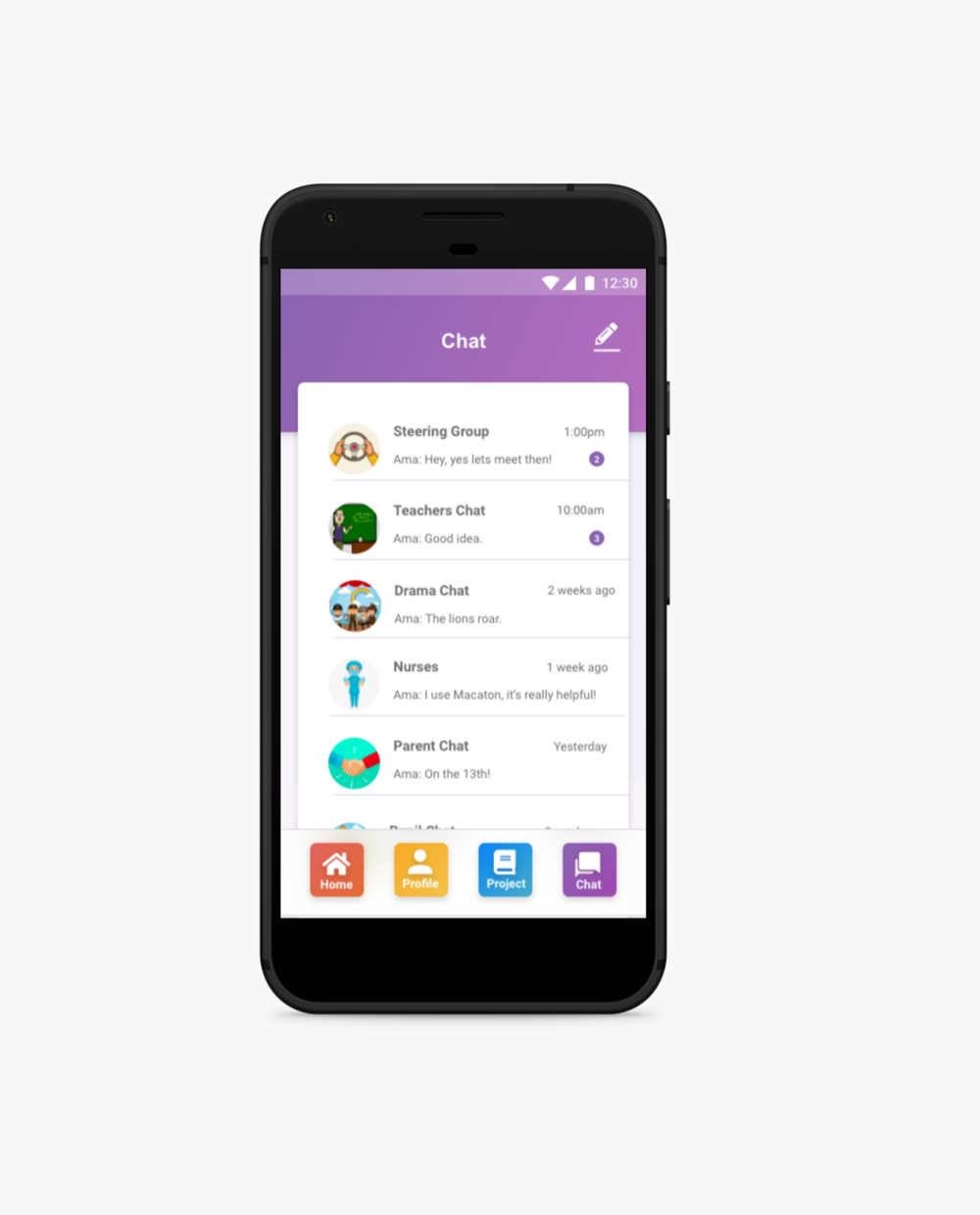
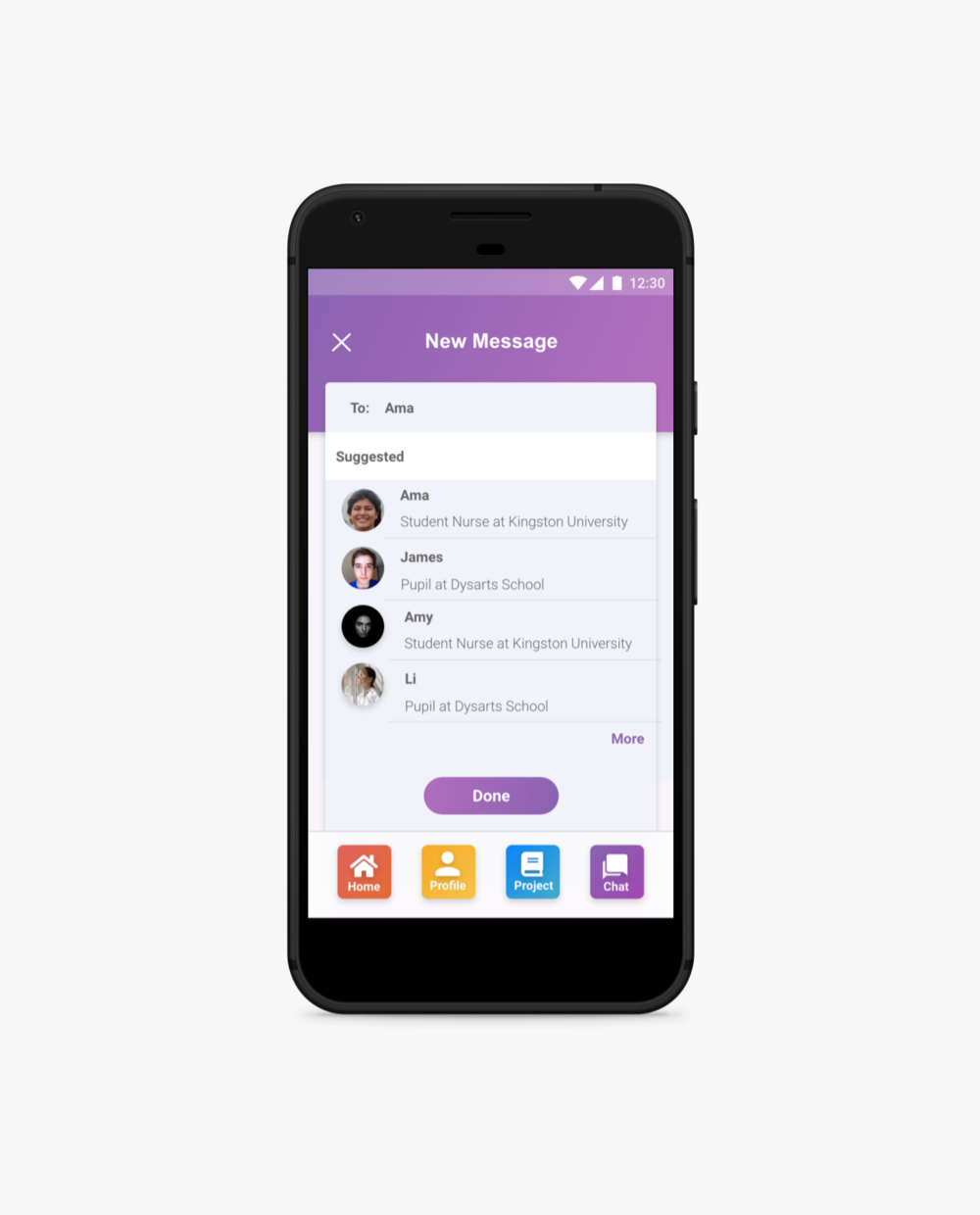
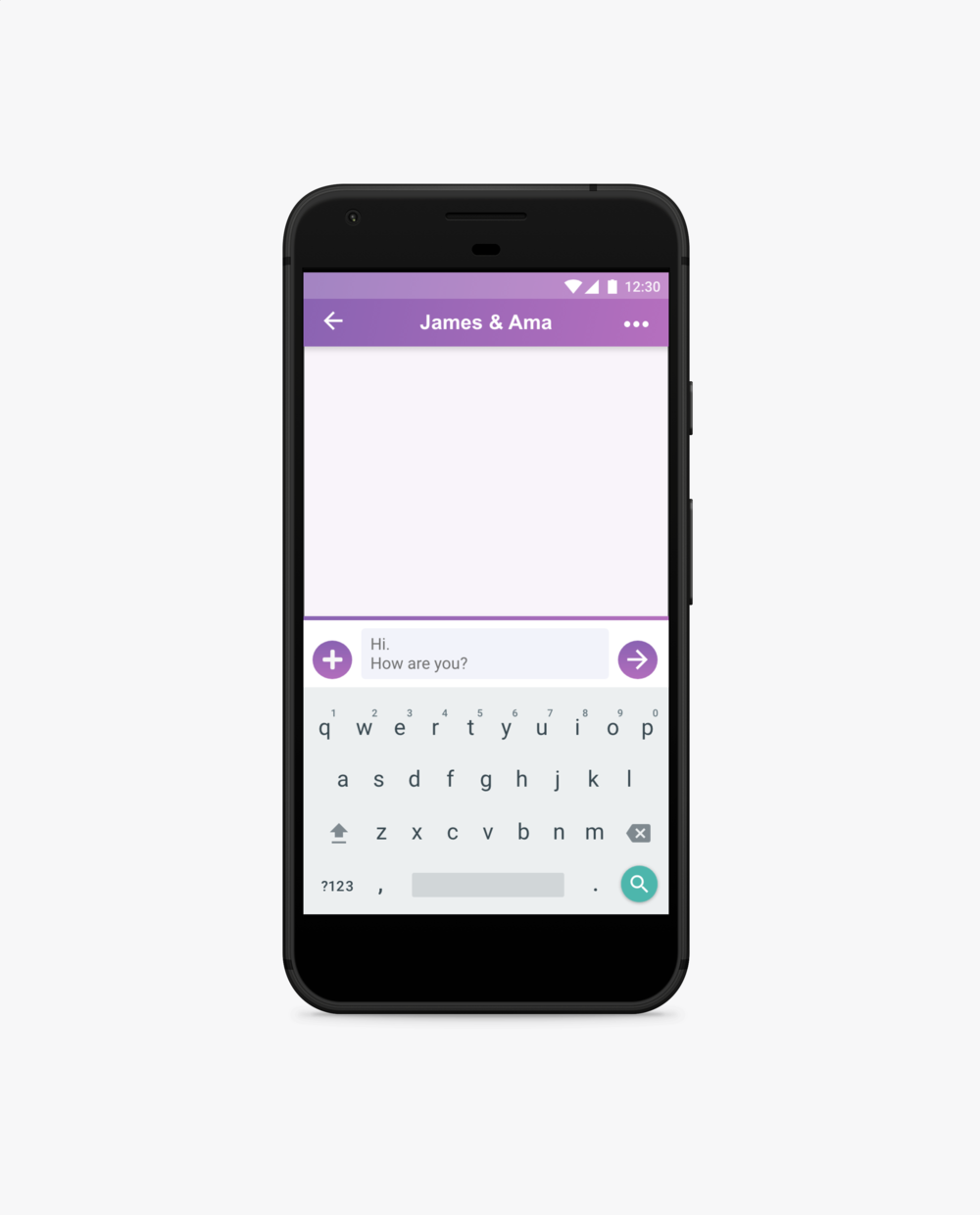
Messaging Platform
Replaced fragmented, last-minute information sharing with a single, clear communication channel. Designed to industry-standard patterns to ensure familiarity and ease of use across all user groups.
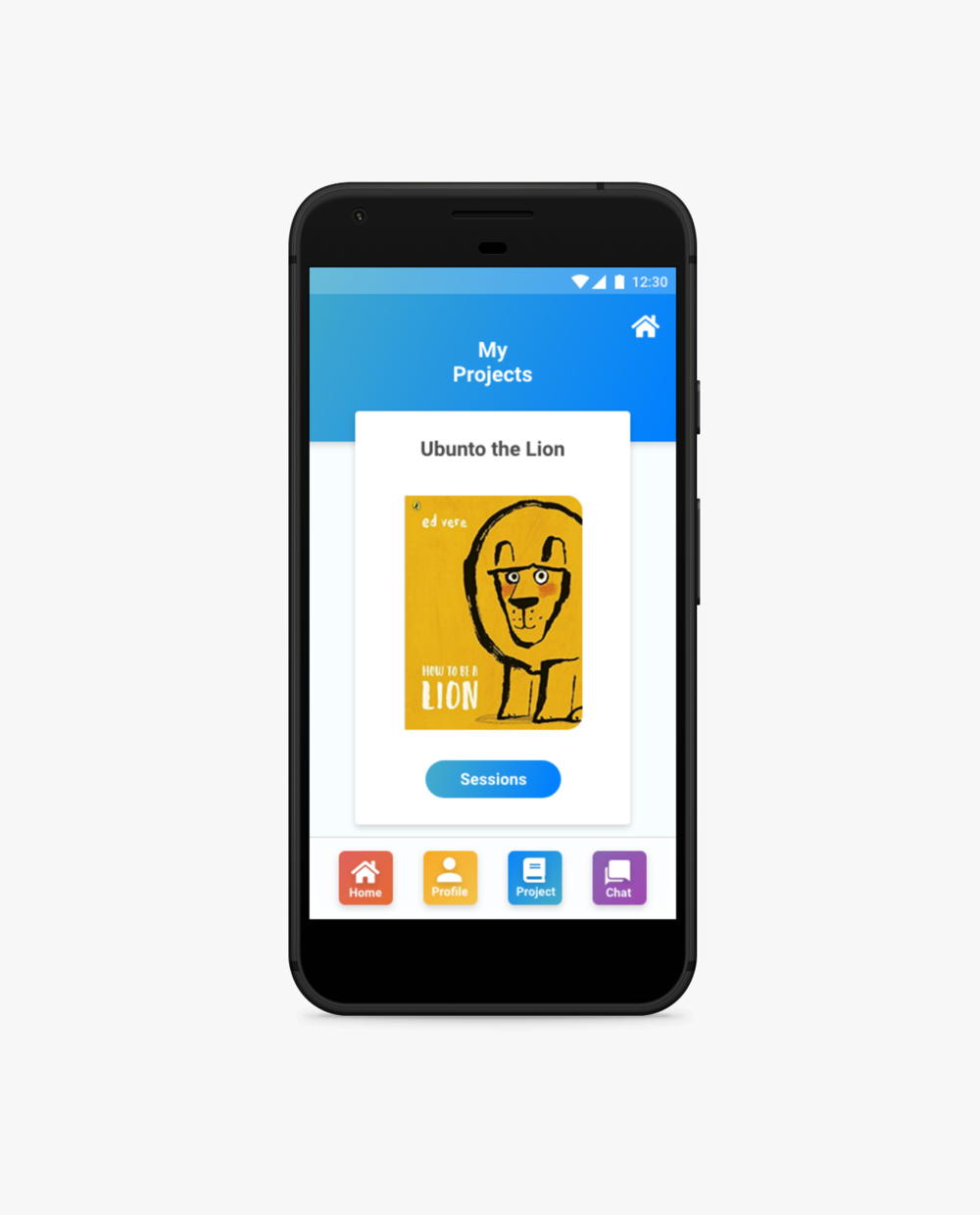
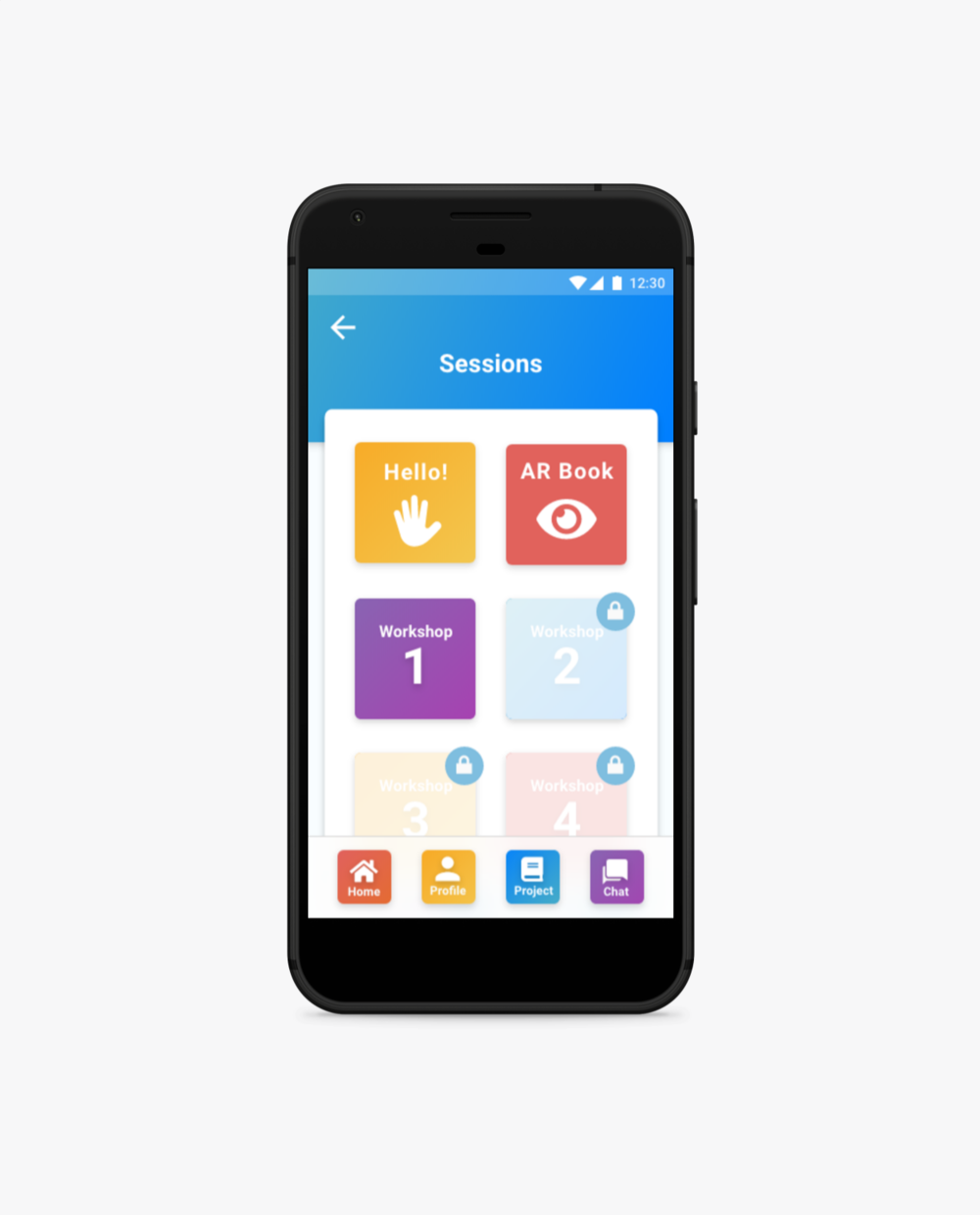
Digital Story Section
Gave children access to the drama group's story ahead of sessions, complemented by visual aids to support preparation and reduce anxiety. An audio element was added so the story could be read aloud — removing a significant barrier for children with complex needs.
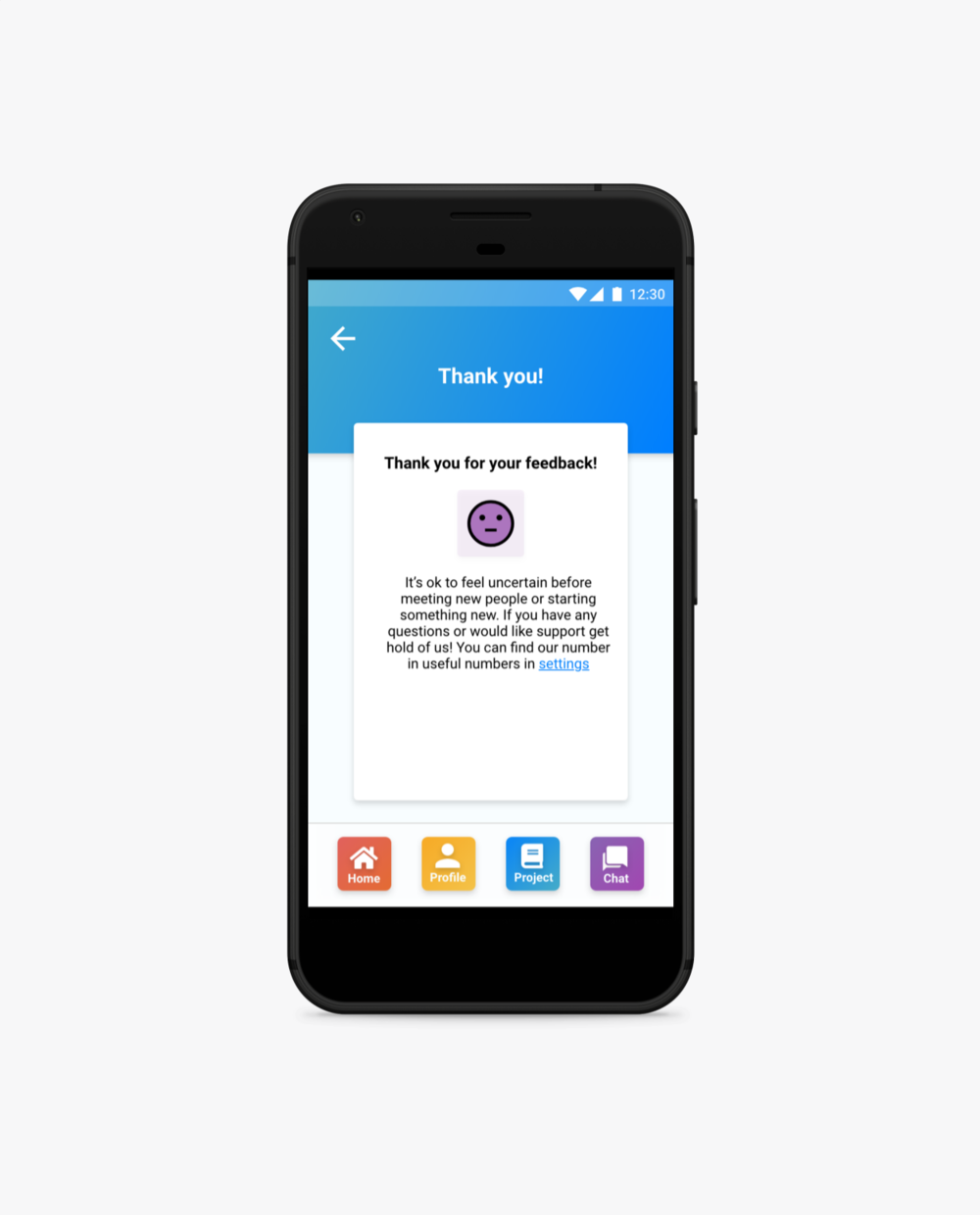
06 — outcome
The final app was approved by Kingston University and secured the roll to the University of East Anglia to take the programme forward — a first step toward the organisation’s ambition of embedding the initiative into nursing syllabuses across the UK.
The project was handed over to another UX designer to test the MVP within the next drama session, with a tablet-optimised version.
07 — reflection
Managing scope with a client who had deep personal investment in the cause required ongoing, clear communication. Framing decisions around research evidence — rather than preference or enthusiasm — was what kept the project on track. I’d invest even more time upfront in establishing shared criteria for MVP scope.
The chat feature was the biggest design lesson. Earlier in my career I felt the need to create something original rather than lean on established interface conventions. Testing quickly showed that familiar patterns exist for good reason — users rely on them. It’s a principle I’ve carried into every project since.
Covid also shaped the research in ways worth acknowledging. Direct testing with the children wasn’t possible, so usability sessions were conducted with disability nursing experts instead. Valuable — but testing directly with the children themselves remains the right next step when circumstances allow.